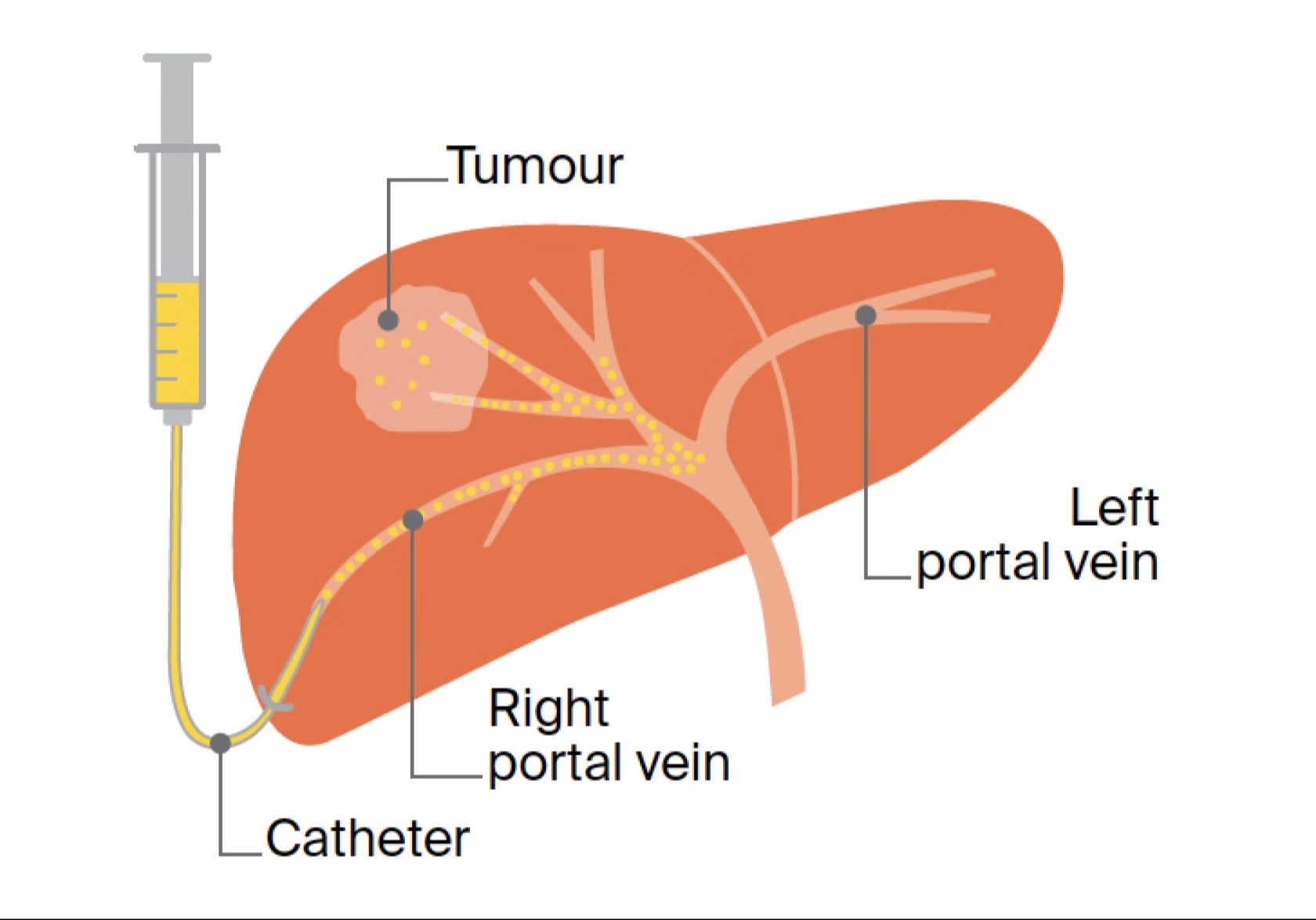
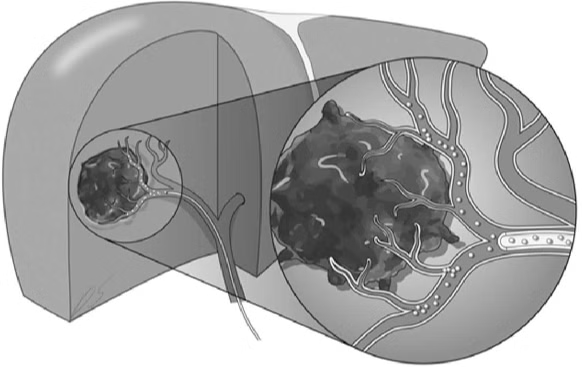
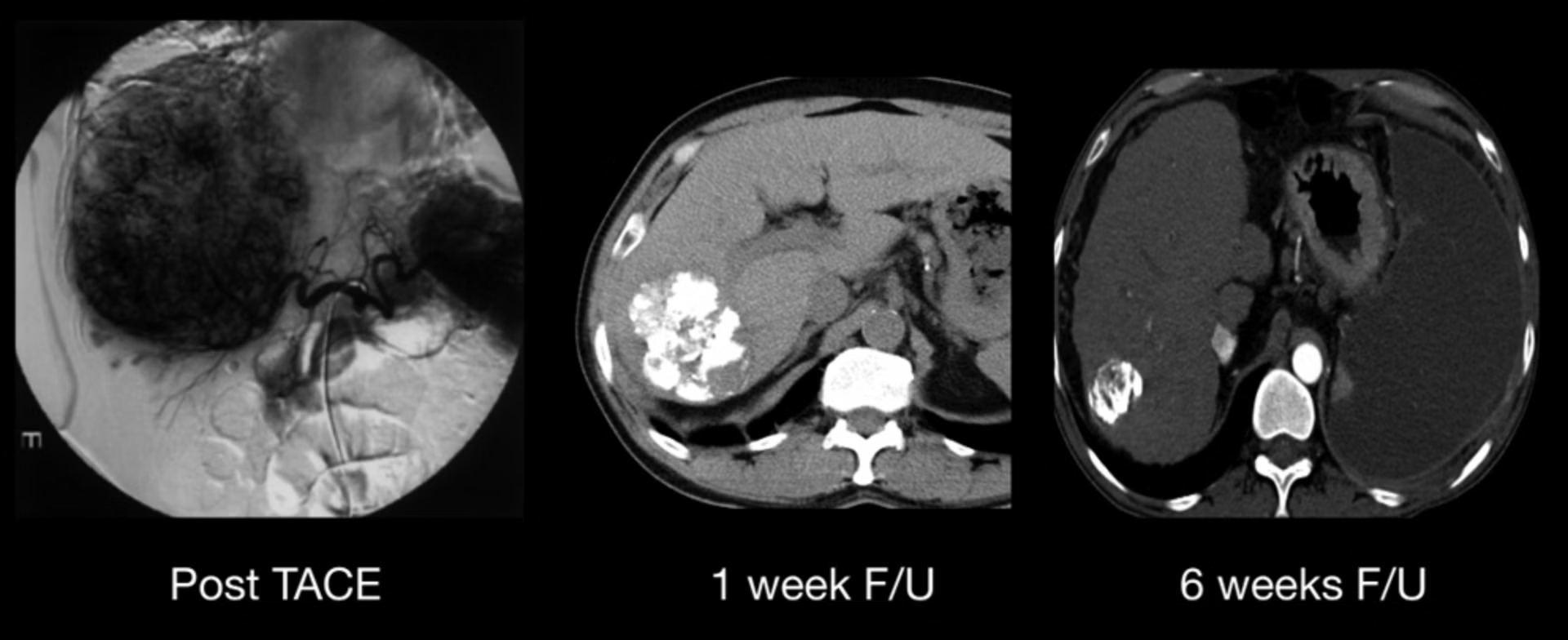
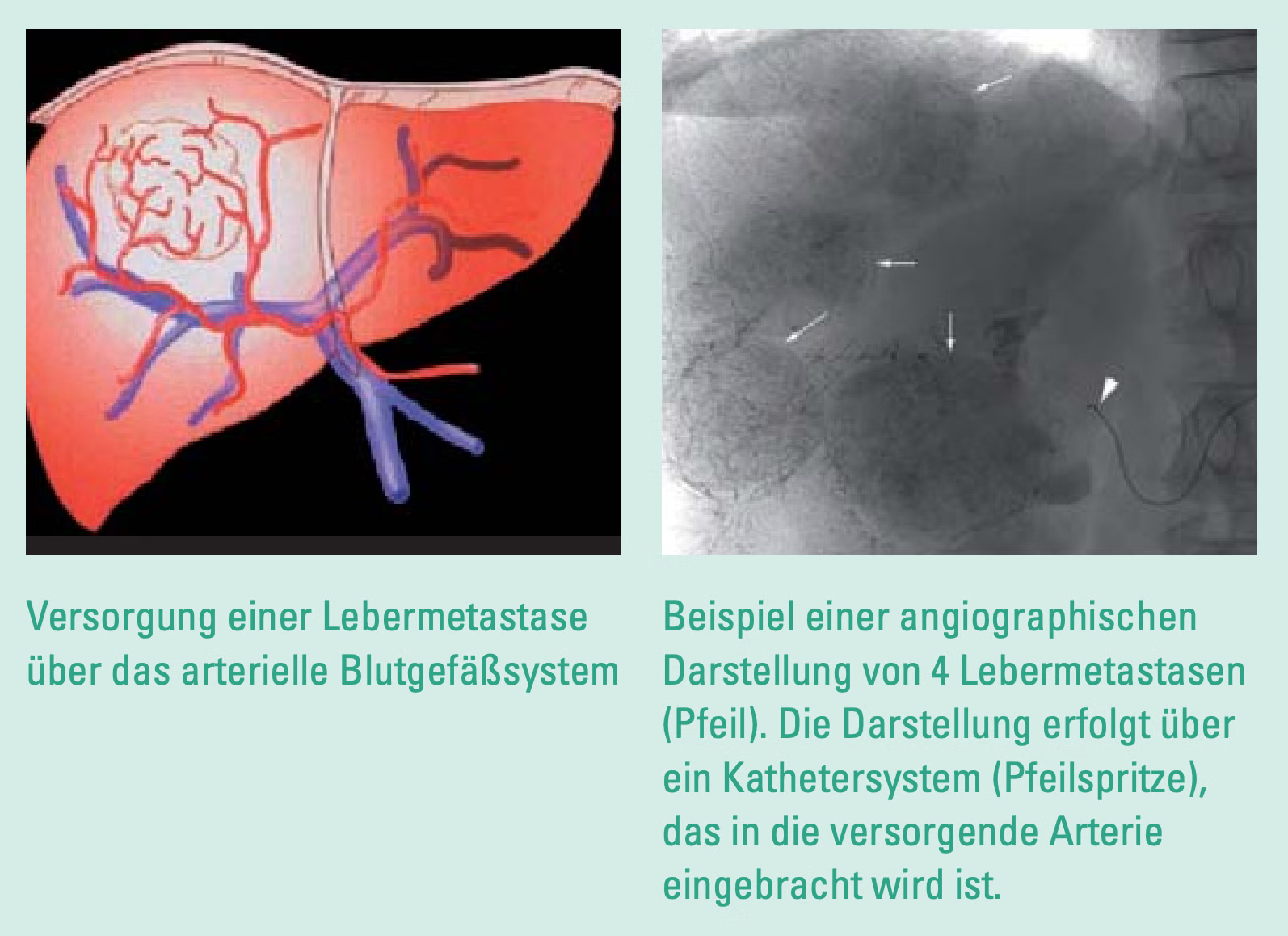
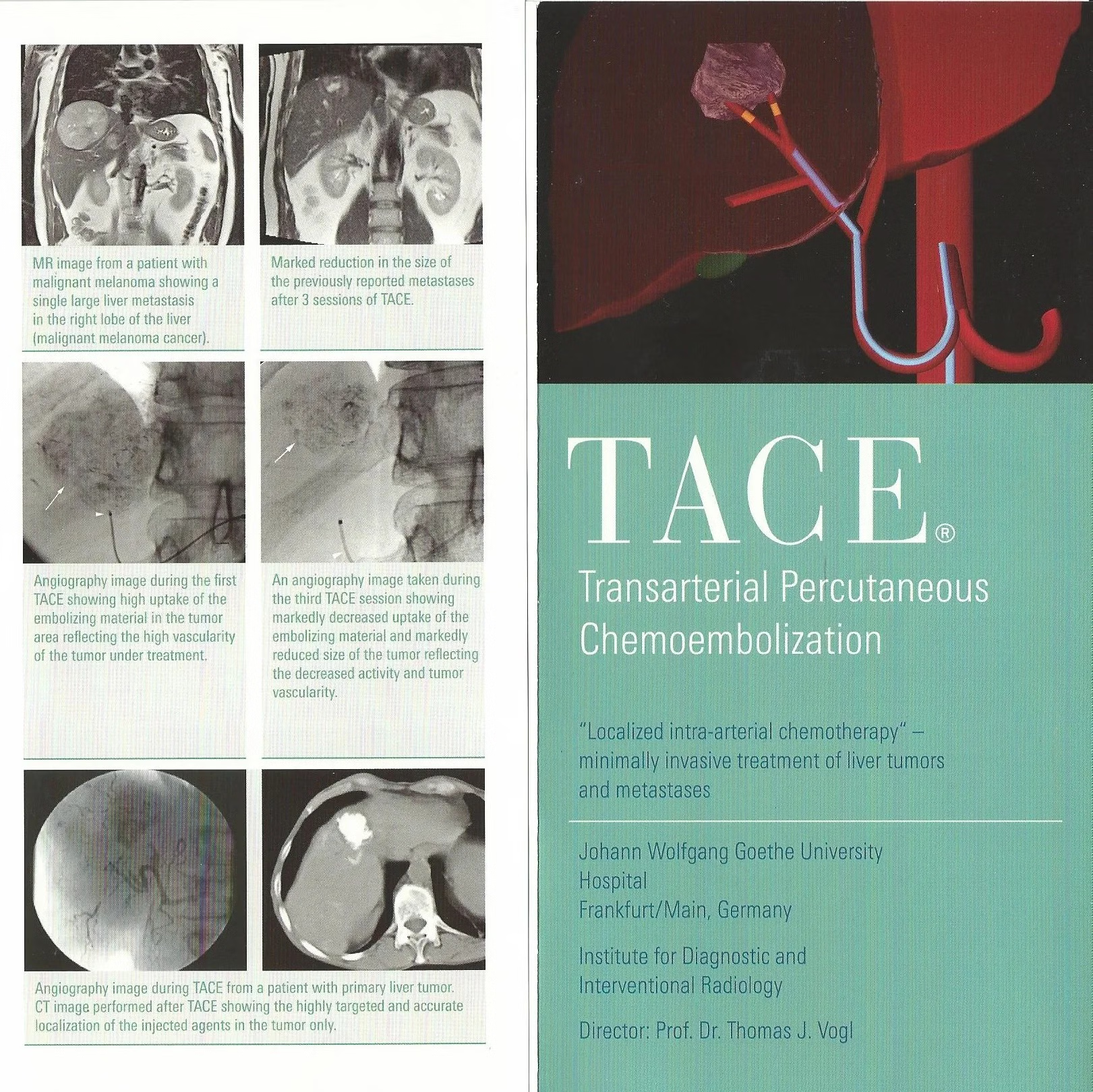
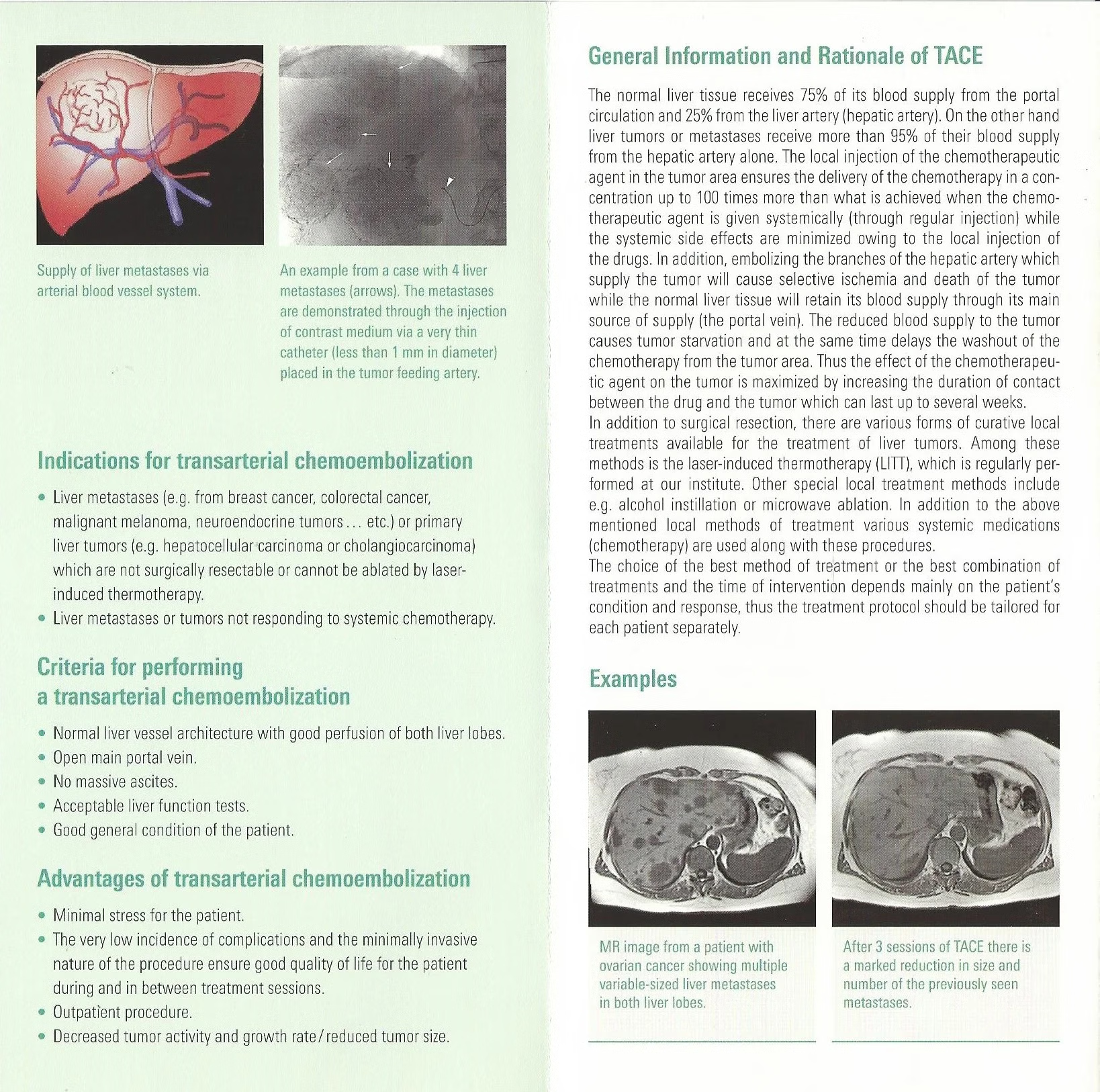
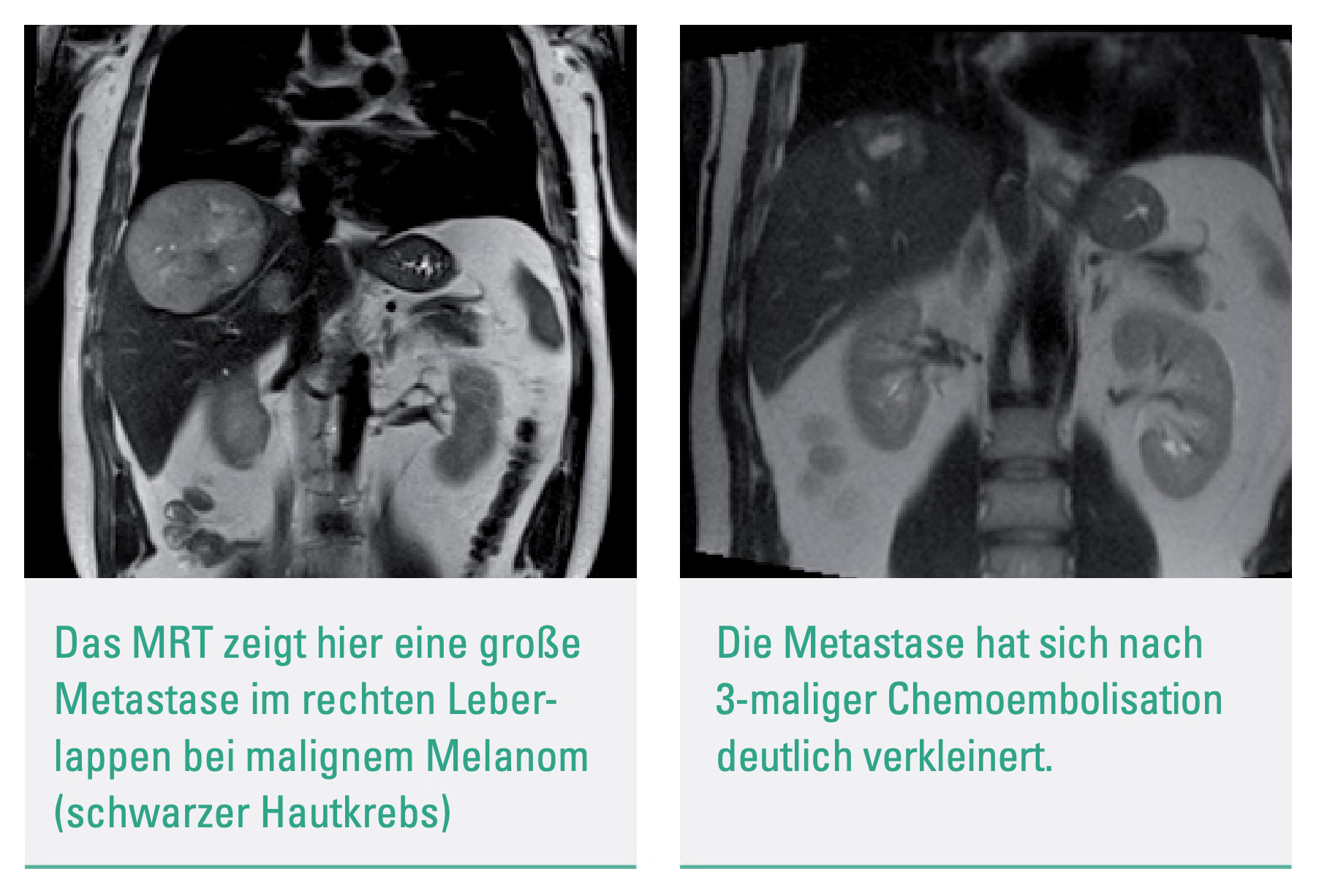
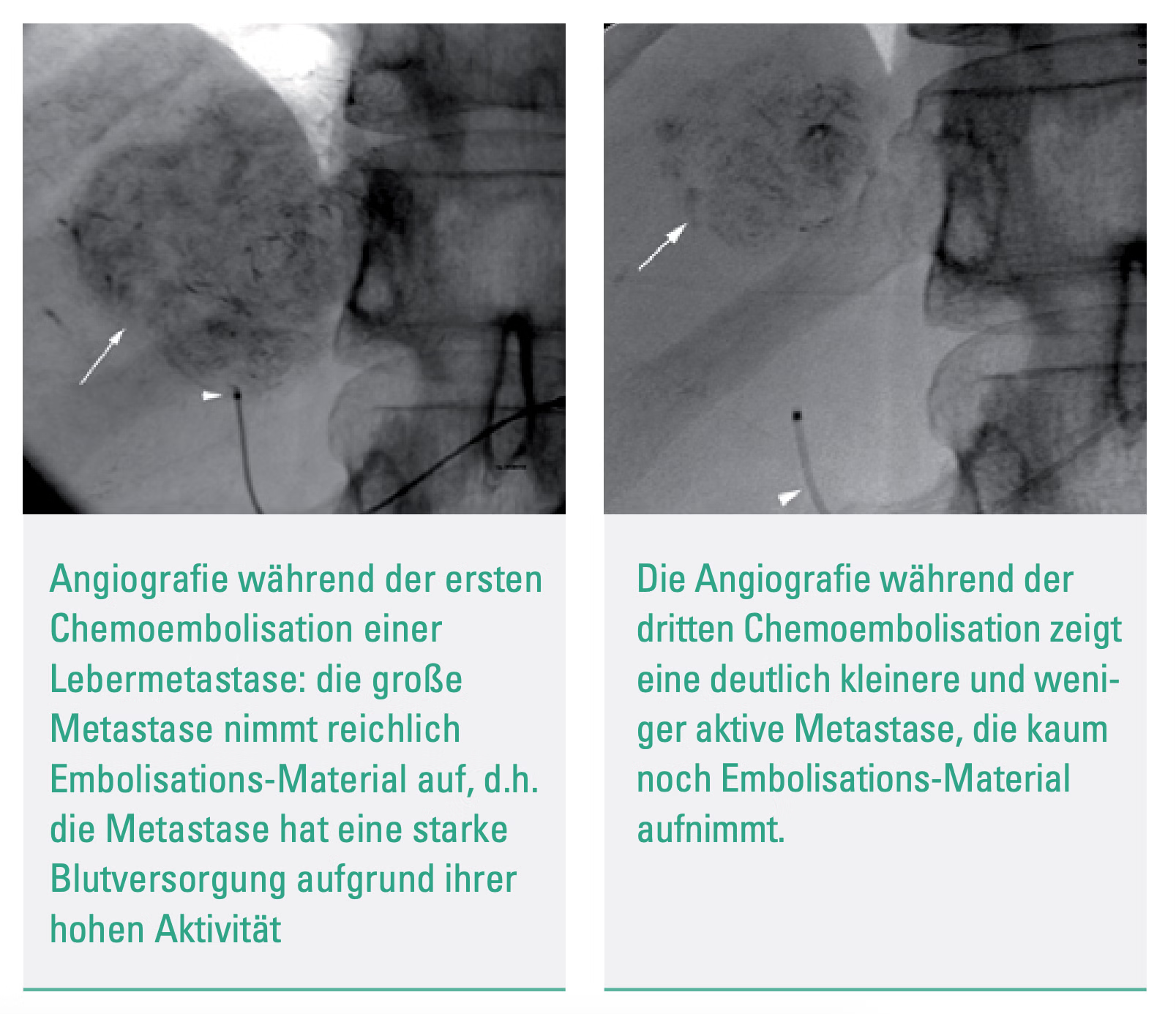
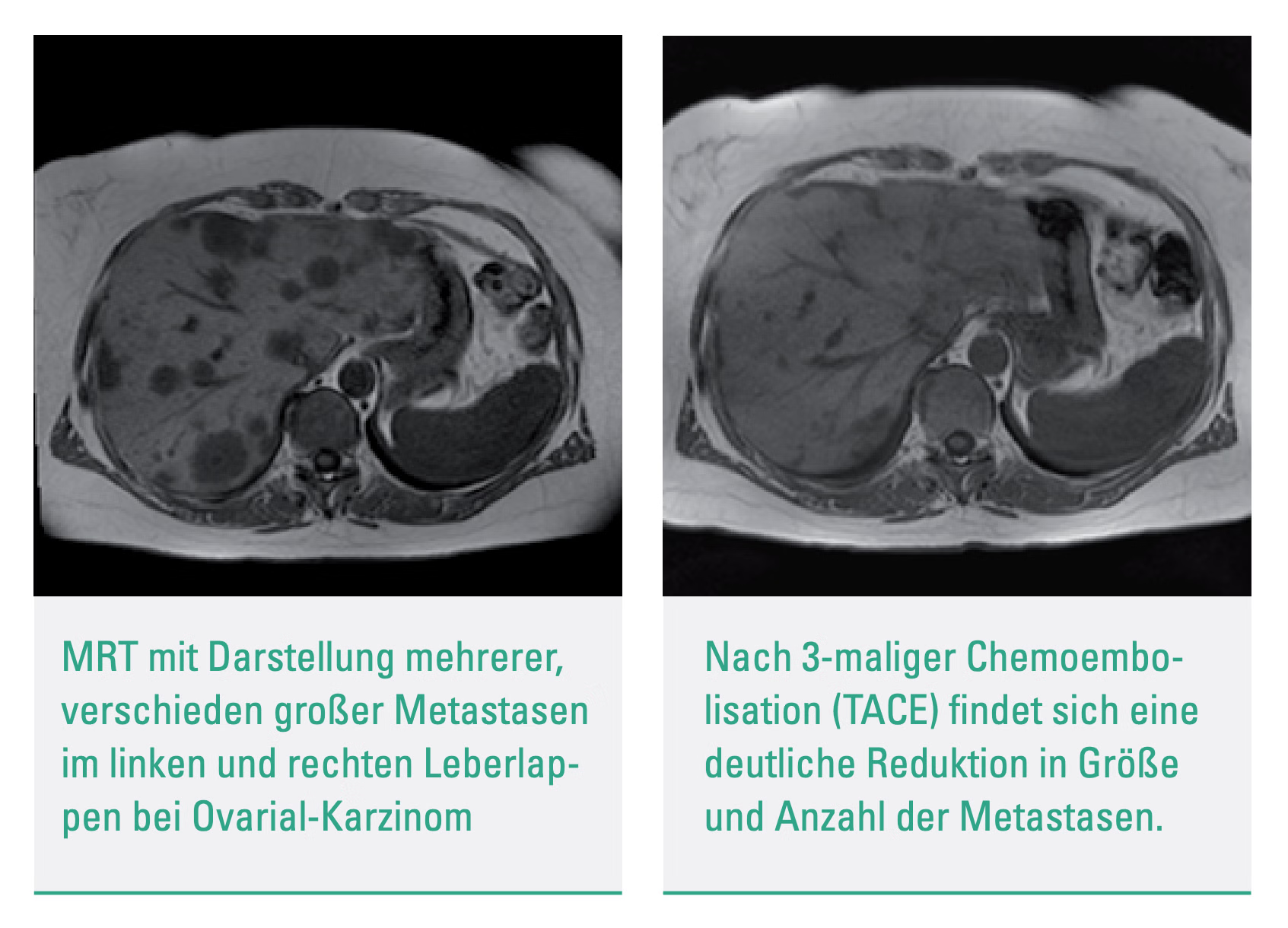
Transarterial chemoembolization (TACE) is the targeted type of advanced and high-dose chemotherapy to treat primary or metastatic liver tumors. It is a procedure with a combination of chemotherapy drugs and embolic agents (substances that stop blood flow) sent directly to the tumor through its blood vessels. Before the therapy, a doctor, a so-called interventional radiologist, orders a CT scan of the liver to check the tumor location and plan a TACE course. A thin catheter is put into an artery in the groin during TACE. It is guided to the vessels that feed the tumor. The catheter puts the chemo drugs and embolic agents into the lesion. The embolic agents stop the blood from going to cancer. It helps the chemotherapy drugs stay longer and work better. Most people are sent home the same day after TACE, an outpatient procedure. Depending on the situation and how well the treatment works, it may need to be repeated in a few weeks or months. TACE is usually well tolerated, but it can have some side effects. Some of these are feeling sick, throwing up, and being tired. Less common but more severe side effects include liver or other organ damage and a higher risk of infection. TACE is usually performed with other treatments, like surgery or radiation therapy, to help keep cancer under control and improve the quality of life. The main advantage of chemoembolization is locally delivering a high drug concentration that can't be applied by conventional systemic chemotherapy. Typically, we perform 2 sessions at once but patients might be indicated for further treatment depending on the individual case. PrinciplesThe TACE therapy method is a specialized treatment that involves delivering chemotherapy to a tumor in a selective and regional manner, followed by occlusion to prevent the spread of cancerous cells. The concentration of the chemotherapeutic agent within the tumor and the arterial hypervascularization of the tumor are the critical parameters that determine the degree of tumor destruction. This method combines chemotherapy and ischemia to achieve maximum tumor necrosis and allows for a higher dose of chemotherapy to be delivered directly to the tumor cells, increasing the contact time between the cytostatic drugs and the cancerous cells. The extent of embolism storage is also an important factor in this method. The healthy liver parenchyma is preserved throughout the procedure. Liver tumors are mainly supplied through the hepatic arteries, while healthy liver tissue receives about 75% of its blood supply from the portal venous system. By embolizing the hepatic arteries, the tumor tissue experiences ischemic necrosis while the healthy liver tissue is preserved due to sufficient portal venous perfusion. The arterial introduction of chemotherapy drugs into the hepatic arteries in the liver tissue achieves up to 100 times higher concentrations than systemic chemotherapy, with fewer side effects. By cutting off the arterial blood flow, the time of action of the chemotherapy drugs is extended, which can range from hours to weeks. TechnologyBefore undergoing chemoembolization treatment, patients are required to fast for at least 6 hours before the procedure. However, they can still take clear liquids or necessary medications up to 2 hours before the treatment. To minimize acute symptoms such as upper abdominal pain or nausea during TACE, patients are given opioids and glucocorticoids through an intravenous route in a standardized manner. Patients are briefed about the procedure's potential side effects and risks before treatment. One of the primary concerns is the likelihood of an embolization syndrome, which can occur in 5-50% of all TACE procedures. This syndrome can lead to several symptoms such as pain, fever, nausea, and vomiting that can last from a few hours to several days. During the angiographic intervention, a pigtail catheter is used to visualize the abdominal aorta, while the celiac trunk and superior mesenteric artery are probed using a cobra or sidewinder catheter. All tumor-supplying arteries and their possible collaterals are then visualized, and indirect splenoportography is done via the superior mesenteric artery and/or splenial artery. These angiographic series aim to show the normal variants of the vessels supplying the liver and to rule out the presence of an arteriovenous or arterioportal shunt, as well as any partial or complete thrombosis of the portal vein. The early arterial and late venous phases from the angiographic series are evaluated to locate the tumor. Depending on the tumor's size, location, and vascular topography, the catheter is then placed either selectively or super-selectively. Using a microcatheter (2. 3-3 F) is recommended to minimize the risk of vasospasm, which is positioned super-selectively in the regional segmental arteries using a coaxial technique. The embolization emulsion is then applied under pulsed fluoroscopy, with reflux into the splenic artery, left gastric artery, gastroduodenal artery, and cystic artery being prevented. Studies show that the survival rates after TACE for patients with vascular anomalies that can be controlled by intervention and collateral circulation are comparable to those with normal topographic conditions. Intervention detailsPrior to the procedure, a digital plan is created using modern imaging techniques to precisely locate the embolisate within the tumor tissue. Following local anesthesia, the femoral artery is punctured using the Seldinger technique. A small 4-F lock is used, with Sidewinder or Kobra catheters utilized for superselective catheterization and chemoembolizate insertion. The chemoembolizate contains mitomycin C, lipiodol, and Spherex. Magnevist is also administered for better contrast. After completion of the transarterial chemoembolization, a pressure bandage is applied and the patient is monitored for 6 hours with regular checks of their blood pressure and pulse rate. The complete TACE treatment includes angiographically guided chemoembolization and a follow-up CT scan without contrast agent 24 to 48 hours after the procedure. Typically, TACE is performed 2-3 times, four weeks apart.
What’s included
Medical service
Examination
clinical history-taking
medical records review
physical examination
consultation with an interventional radiologist
Laboratory tests
complete blood count (CBC)
blood type test (ABO, Rh)
biochemical analysis of blood (kidney and liver function tests, electrolytes)
inflammation blood tests
coagulation studies
urinalysis
Diagnosis
ultrasound imaging of the abdomen
CT scan of the liver with a contrast
post-procedure CT scan of the liver
Treatment
pre-procedure patient preparation
2 sessions of transarterial chemoembolization (TACE) for a liver lesion/tumor
If you're not seeing exactly what you need here, send your custom request. You can discuss the content, specifics, price & timeline to create a personalized plan.
Location
Theodor-Stern-Kai 7, 60596 Frankfurt am Main, Germany
FAQ
What are typical indications for liver TACE?
Liver metastases or primary tumors that are not surgically or thermotherapy resectable and do not respond to systemic chemotherapy, as diagnosed by intraoperative or image morphology by CT or MRI.
What are the requirements?
The liver has normal blood vessels to supply both lobes, an open portal vein, no fluid accumulation in the abdomen, adequate liver function, and the patient is in good general condition.
What are the advantages?
The treatment's benefits include low patient burden, low complication rates, improved quality of life, shorter hospital stays, and reduced tumor growth.